
Development of a Bio-Psycho-Social-Spiritual framework to prevent stress in first responders
Click here to download the pdf
Executive Summary
Background
In Australia 140,300 full-time first responders - Emergency Medical Services (EMS), Police, Ambulance, and Fire - work at the borderline of life and death, in high-risk environments and situations. First responders are also reported to be at a higher risk of serious harm from psychological workplace injuries compared to the general population. In fact, one in three first responders experience high or very high psychological distress compared to one in eight in all adults in Australia. During the COVID-19 pandemic, it has been further reported that first responders’ rates of depression were ten times higher than the general population while rates of anxiety were four times higher. This comes at a great human cost to communities, and large financial cost to governments. Serious mental disorder claims among first responders account for 9.9% of all mental disorder related workers compensation claims in Australia, but account for 18.3% of the total cost of mental disorder payments. Consequently, every first responder organisation in the country has engaged multiple discipline wellbeing teams (MDWTs) to address this increased risk of psychological harm. However, despite the delivery of mental health interventions to first responders by MDWTs, the expected reductions of serious workers’ compensation claims for mental disorder have not been observed.
Treatment and prevention of psychological distress among first responders
A review of the literature showed that current approaches utilised by MDWTs for the treatment and prevention of psychological harm experienced by first responders are based on the dominant biopsychosocial framework. Through a biopsychosocial lens, MDWTs typically deliver to first responders secondary and tertiary intervention strategies that target individuals. The current strategies include clinical and therapeutic regimes that almost exclusively address posttraumatic stress disorder (PTSD) that is believed to arise from trauma exposure.
There is growing concern that there is an over-emphasis on trauma exposure as the cause of psychological harm whilst workplace stressors have been largely overlooked as a source of distress. A key point of concern is that interventions based on the biopsychosocial framework do not generally include matters of spirituality that have been found to better address psychological harm caused by moral suffering that consider both traumatic events and organisational stressors. Moral suffering arises when one’s just world beliefs are breached by the actions of others or oneself and can lead to guilt, shame, outrage, suicidal behaviours and workplace deviance. Moral suffering has been extensively researched in military populations, while research in first responder contexts is in its infancy.
In addition, the clinical and therapeutic focus of current interventions neglects a work, health, and safety (WHS) lens which promotes true primary prevention strategies for psychological distress by identifying, assessing, and controlling psychological hazards. Not surprisingly, interventions based on the clinical and therapeutic biopsychosocial model have not reduced the incidence of distress to the degree that might have been expected. In summary, the main points revealed by the literature review were:
- lack of research around first responders and moral suffering, despite exponentially increasing research in the military context;
- over-emphasis by first responder wellbeing programs on the content of first responder work, namely trauma exposure, as the cause of distress;
- over-emphasis by wellbeing programs on individual focussed interventions at the expense of interventions that address organisational causes of distress;
- lack of attention to religious/spiritual (R/S) or existential struggles and their spiritual solutions due to the use of a limited biopsychosocial framework;
- lack of precision in identifying the kinds of events and cultures that can cause moral suffering in non-military contexts;
- lack of a WHS lens to produce truly primary prevention strategies based on psychological hazard, identification, assessment, and elimination.
Research aims
The purpose of this study was to empirically develop a framework to address the psychological distress that can arise in first responders from exposure to potentially morally injurious events (PMIEs). The primary research question was:
“What features can be incorporated into the current biopsychosocial model in order to address moral suffering and to create a biopsychosocial-spiritual model?”
However, before answering the above question and creating a biopsychosocial model, researchers needed to ascertain that moral suffering is, indeed, a significant issue needing to be addressed among Australian first responders, which led to the followings secondary research questions:
- “What is the extent to which Australian first responders are exposed and affected by moral suffering?”
- “How is reported moral suffering connected to spirituality?”
- “What are the types of moral suffering to which first responders are exposed?”
- “What is the impact on meaning-making and identity from events connected to moral suffering?
- “What types of organisational practices and cultures contribute to moral suffering?”
- “What do first responder organisations know about moral injury and moral suffering?”
- “How do first responder organisations see moral suffering fitting into their existing wellbeing practices?”
To address the finding that matters of spirituality better address psychological harm caused by moral suffering the following research question was also included in the study:
“In what way does a theological perspective illuminate, interrogate, and suggest alternative ways of acting in response to the collected data?”
Method
To answer the above research questions, a mixed-method approach combining quantitative and qualitative approaches and Practical Theological Reflection (PTR) was employed:
- Quantitative - Bayesian Network analysis of surveys from 229 Australian first responders was used to gain insight into the nature and extent of moral suffering among first responders and also into how reported moral suffering is connected to spirituality. To assess moral suffering three psychometric scales that measured “moral distress”, “moral injury”, and “perceived injustice” were administered;
- Qualitative (part 1) - narrative analysis of 21 existing auto/biographies that detail the experiences of first responders was conducted to gain in-depth understanding of moral suffering among first responders and of how it is connected to spirituality;
- Qualitative (part 2) - narrative analysis of semi-structured interviews with 16 authors of the auto/biographies was conducted to gain in-depth understanding of moral suffering among first responders; and
- PTR - to gain insight into spiritual practices that may be useful in preventing any moral suffering identified in the qualitative and quantitative analyses.
Results
Quantitative analyses
Statistical analysis of survey responses from first responders was conducted to gain insight into the nature and extent of moral suffering among first responders and also into how reported moral suffering is connected to spirituality. The quantitative data revealed that moral suffering is present in first responders at moderate to high rates. A total of 85 first responders (37.12%) reported having felt betrayed by a manager, colleague, or systems/people in their organisations over 50 times during their careers. Those who reported higher levels of betrayal also reported higher levels of moral suffering.
The elements of all three scales (moral distress, moral injury, and perceived injustice) were reported to be moderate to high in all occupation groups of first responders. Importantly, of particular note from the quantitative study (survey results) was the consistent presence of perceptions of betrayal and attributions of blame in first responders. Indeed, cognitions of blame against individuals who believed to be responsible for their moral suffering were found to be high in the current study. For instance, police reported prevalence rates of clinically significant distress due to perceived injustice at rates equal to those with serious injuries from motor vehicle or industrial accidents. Therefore, moral suffering is a concept that must be considered in any program that aims to reduce psychological distress in first responders.
Further, the quantitative data showed a direct relationship between spirituality and moral suffering. When participants’ religiosity or spirituality declined, it was associated with elevated levels of moral suffering, as measured by all three scales. Those who reported the lowest levels of moral suffering reported either stable or some growth in religiosity and/or spirituality (R/S). The experience of increased perceived injustice was the form of moral suffering most significantly associated with spiritual decline, while spiritual growth was associated with lower levels of perceived injustice.
Qualitative analyses
As mentioned above, qualitative analyses were conducted to gain in-depth understanding of moral suffering among first responders and of how it is connected to spirituality. The qualitative analysis found that moral suffering was evident in participants who experienced betrayal, leaving them feeling conflicted, detached from their own emotions and other people, or feeling abandoned by leaders and organisations. It was also found that the rigorous selection and training of first responders can lead to the perception that they are strong or invulnerable to harm. However, due to the traumatic nature of their work, they have been found to have an ironic vulnerability to harm. In addition, qualitative results pointed to symptom manifestation among first responders that are consistent with moral injury, such as shame, anger, exhaustion, moral dissonance, sense of abandonment and betrayal, personal identity challenges, suicidality, substance abuse, and harm to personal relationships outside work.
The types of events most often described by qualitative research participants as causing harm included poor resourcing, work overload, trauma in vulnerable groups, lack of appropriate recognition, organisational injustice, and poor support from leaders. Such themes reported by first responders largely overlapped with psychosocial hazards identified in the workplace psychosocial hazard guidelines that were released by SafeWork NSW in 2022. However, moral suffering and psychosocial hazards have not generally been considered together for the purpose of reducing psychological harm in the workplace.
Practical theological reflection
Finally, a Practical Theology Reflection (PTR) was enacted on the sum of the data collected in the qualitative and quantitative methods above. The purpose of this theological reflection was to gain insight into spiritual practices that may be useful in preventing any moral suffering identified in the qualitative and quantitative data analyses. Based on the quantitative and qualitative analyses, the two important themes that were subject of the PTR were the nature and response to betrayal, i.e., response to experiencing an injustice at work or to witnessing one, and the need for supportive leadership within a secular spiritual framework. The main themes that arose from the PTR were:
- The need for forgiveness and restoration in the workplace
- The power of listening to employees
- The need for individuals to learn to examine their own behaviours
- Moral imagination (People are asked to “examine themselves” to take responsibility for their own character and asked to exercise one’s “moral imagination”)
- Enlarged thinking (People are encouraged not to jump to conclusions by “taking the log out of one’s own eye,” a common biblical concept that describes being aware of one’s own faults before casting judgement on others)
- Leadership of ironic vulnerability (Leaders must recognise the vulnerability of worker in first responder organisations who have a high trauma load)
- Addressing moral suffering through key leadership behaviours
- Strong leadership that displays vision, authority, and sincerity,
- A servant hearted, sacrificial attitude,
- Filial and gracious physical presence with those they lead,
- Two-way communication that values active listening, asking, and truth-telling,
- The provision of physical and emotional needs of worker and facilitate pastoral care,
- Protection of staff from harassment and organisational injustice,
- Regular expression of gratitude to staff as enacted thankfulness,
- Restoration and renewal of staff after wrongdoing, error, or conflict,
- Continuing to be the follower of a higher authority.
Industry outreach activities
Also noteworthy, informal industry outreach was conducted to provide insight into first responder organisations’ perception and willingness to adopt a biopsychosocial-spiritual model. Forty-five representatives of first responder organisations across Australia and internationally were consulted. Such consultations showed there was a lack of understanding about moral suffering and its role in psychological distress among first responder organisations. Not a single organisation had programs in place that addressed moral suffering. Consistent with the literature review findings, all organisations were primarily focused on the delivery of interventions to treat trauma exposure.
In addition, it was also found that psychological contracts that first responder organisations had with employees can be a source of tension and distress. For example, participants noted that many first responder recruitment campaigns present implicit promises of adventure and excitement where workers do something “worthwhile.” However, when work is regularly mundane or apparently meaningless it can have a negative impact on the perception of the organisation by workers.
Finally, during consultations participants expressed concerns about the lack of unity among different professional groups that compose MDWTs. Rivalry among professional groups appeared to be the rule rather than an exception.
Discussion
The current study investigated the adoption of a BPSS framework to prevent moral suffering among first responders. Results from quantitative and qualitative analyses showed that a BPSS framework can assist first responder organisations to meet their obligations to control psychosocial hazards. A BPSS framework provides a vital bridge between moral suffering and psychosocial hazard reduction, as it provides the basis for the delivery of intervention strategies for preventing psychologically and spiritually harmful behaviour in the workplace.
Moreover, the good news is that organisational, clinical, and pastoral responses to moral suffering can potentially be enhanced by the elimination of the events identified in the current study that can be perceived as betrayal. Therefore, based on a BPSS framework, first responder organisations may profit from a set of truly holistic intervention strategies aimed at eliminating such events.
The moral suffering identified in the current study in the form of blame cognitions and sense of organisational betrayal often led to feelings of anger and even a desire for revenge that must be addressed through intervention strategies if a mentally healthy workplace is to be created. Intervention strategies that help to alter the individual’s perceptions of betrayal and lead to the possibility of forgiveness and reconciliation are important in the creation of such a mentally healthy workplace, as they address maladaptive anger and retribution. That is, intervention strategies( in accordance with the findings from the PTR) that take into account moral suffering and the spiritual element that is used to prevent and treat it. No doubt, effective implementation of such intervention strategies may assist in preventing counterproductive workplace behaviours, such as absenteeism, risk taking, and inappropriate or criminal behaviour that arise as acts of revenge for perceived injustices. Indeed, the observation that poor organisational citizenship can be motivated by the desire to seek revenge for betrayal means that addressing spirituality and moral suffering through intervention strategies based on the findings from the PTR will bring benefits for first responder organisations by potentially reducing motivation for misconduct.
Indeed, the PTR indicates that the spiritually based intervention strategies can create practical and spiritually grounded cultures and practices potentially capable of eliminating the reported psychological harmful PMIEs thereby preventing moral suffering. Given that many of the causes of moral suffering include modifiable organisational or leadership practices, this BPSS model proposes 4 preventative interventions that potentially eliminate harmful betrayals that directly minimise the impact of blame cognitions reported in the current study. Figure 1 summarises the reported causes of moral suffering (green circles) and the fourfold interventions (orange boxes) of the BPSS framework.
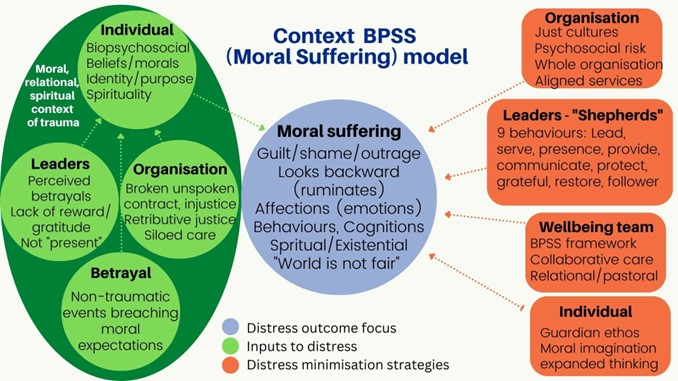
Figure 1. Conceptual model of the BPSS framework.
Conclusion
The findings of this research highlight the experiential and existential dimensions of moral suffering that occurs in first responders and how to prevent it. Future research may be able to test and refine the elements of this model for use in different cultural and organisational settings. Addressing the organisational factors that contribute to distress may produce a healthier and more cost-efficient workplace in the high-risk community of first responders. Additionally, the BPSS framework will help organisations meet their requirements under emerging psychosocial safety legislation.
Click here to download the pdf